
CO 197 Denial Code is a common healthcare claim denial that indicates the payment has been reduced or denied because the service provided is not covered under the patient’s insurance plan or does not meet the payer’s coverage requirements. Medical billing teams must review the denial carefully to determine whether the claim should be corrected, appealed, or billed to the patient according to payer guidelines.
What Is the CO 197 Denial Code?

In plain English, CO 197 means your insurance company didn’t get the green light it needed before you provided a service.
This code comes from X12, the official organization that maintains billing codes for the entire U.S. healthcare industry. Their exact wording for code 197 is “Precertification/authorization/notification/pre-treatment absent.”
Translation? The payer is saying: “You needed our approval first, and we never got it. So we’re not paying.”
This denial falls under a bigger category called a Claim Adjustment Reason Code, or CARC for short. Think of CARCs as the official reasons insurance companies use to explain why they didn’t pay a claim the way it was billed. CO 197 is simply one entry on that long list.
What Does “CO” Mean in CO 197?
Every denial code starts with a two-letter prefix, and that prefix changes everything about who pays the bill.
“CO” stands for Contractual Obligation. It means the denial exists because of the agreement between you and the insurance company, not because of anything the patient did wrong.
Here’s why that matters so much: with a CO denial, you cannot bill the patient. Your contract with that insurer already spells out the rules, and missing authorization is on you, the provider, to fix.
Compare that to a PR (Patient Responsibility) code. If the same denial showed up as PR 197 instead, the patient could be billed directly. Same root cause, completely different financial outcome.
We’ll dig deeper into that difference in just a moment.
Common Causes of a CO 197 Denial

Most CO 197 denials trace back to one of these situations. Some are simple mistakes. Others are timing issues that catch even experienced billing teams off guard.
- Prior authorization was never requested before the service happened
- Authorization was requested but not approved in time, and the service went ahead anyway
- The authorization number was entered incorrectly on the claim
- Authorization expired before the service was actually performed
- Notification requirements were missed for services that need advance notice instead of full authorization
- Documentation didn’t support medical necessity, so the request was never properly processed
- A required second opinion wasn’t obtained when the plan demanded one
- The wrong procedure code was billed, so it didn’t match what was actually authorized
Notice a pattern here? Almost every single cause traces back to timing and verification, not the quality of care provided.
That distinction matters. A CO 197 denial doesn’t mean you did anything medically wrong. It means a piece of paperwork didn’t line up with a deadline.
CO 197 vs. PR 197 What’s the Difference?
This is the question that trips up even seasoned billers, so let’s settle it once and for all with a clear comparison.
| Factor | CO 197 | PR 197 |
| Who pays | The provider absorbs the cost | The patient can be billed |
| Root cause | Missing authorization, provider’s responsibility | Missing authorization, but patient didn’t meet a plan requirement |
| Can you appeal? | Yes, with documentation | Yes, but outcome depends on patient’s plan terms |
| Most common in | Provider-side authorization failures | Plans requiring patient self-notification |
The number “197” means the exact same thing in both cases: authorization was missing. What changes is who’s financially responsible for that gap.
If you see PR 197 instead of CO 197, don’t assume it’s an error. Double-check your payer’s specific policy, because some plans genuinely do shift this responsibility to the patient under certain circumstances.
Understanding the Remark Codes Behind CO 197

Here’s something almost nobody talks about: CO 197 rarely shows up alone. It travels with a remark code that gives you extra clues about what exactly went wrong.
Think of the denial code as the “what” and the remark code as the “why” or “what to do next.”
| Remark Code | What It Means | Your Next Move |
| N210 | Alert: You may appeal this decision | Gather documentation and submit a formal appeal |
| MA120 | No authorization on file at all | Check if authorization was ever requested; submit a retroactive request if possible |
| M62 | Authorization may exist but wasn’t transmitted correctly | Verify the authorization number and resubmit with corrected information |
Why This Matters More Than You Think
Skipping the remark code is like reading half a sentence. You’ll know something went wrong, but you won’t know exactly how to fix it.
Always check the remark code paired with your CO 197 denial before you decide on your next step.
How Do You Fix a CO 197 Denial?
Good news: this is a fixable problem, and most claims with this denial can absolutely get paid.
Follow these steps in order:
- Pull up the original claim and remittance advice. Confirm the exact remark code attached to your CO 197 denial.
- Check your system for any existing authorization. Search notes, uploaded documents, and prior communications with the payer.
- Verify the authorization number is correct. A single transposed digit can trigger this entire denial.
- Contact the payer directly if you can’t locate any record of authorization on your end.
- Request retroactive authorization if your payer’s policy allows it. Many do, especially for emergency or urgent situations.
- Correct and resubmit the claim with the proper authorization number included.
- If billing on a CMS-1500 form, place the authorization number in Item 23.
- If billing electronically, include it in loop 2300 or loop 2400, using the correct reference qualifier.
Most claims that get fixed at this stage never need to go further. But sometimes, you’ll need to appeal instead.
How to Appeal a CO 197 Denial
If retroactive authorization isn’t an option, or the payer denies your correction, it’s time to appeal.
An appeal is your formal request asking the insurance company to reconsider its decision. Done right, it works far more often than people expect.
What to Include in Your Appeal Letter
- The claim number and patient information, clearly stated at the top
- A direct explanation of why authorization wasn’t obtained
- Supporting medical documentation proving the service was necessary
- Any communication records showing you attempted to get authorization
- A clear, polite request for reconsideration and payment
- Keep your tone professional and factual. Insurance reviewers respond better to clear documentation than to frustration, even when frustration is completely justified.
How to Prevent Future CO 197 Denials
The best fix is the one you never need. Here’s how billing teams cut these denials down dramatically.
- Build a pre-service verification checklist that flags every procedure code requiring authorization
- Set authorization reminders tied to expiration dates, not just request dates
- Automate eligibility and authorization checks wherever your software allows it
- Train front-desk and scheduling staff to catch authorization gaps before the appointment even happens
- Track your CO 197 denial rate monthly so you catch patterns early instead of after they’ve cost you thousands
One study-backed fact worth knowing: prior authorization remains one of the top administrative burdens reported by physician practices nationwide, according to American Medical Association survey data. You’re not imagining how disruptive this process feels. It’s a real, widely documented pain point across the entire industry.
Real-World Example: How a CO 197 Denial Happens
Let’s make this concrete with a scenario pulled straight from a typical billing week.
A patient comes in for an MRI to investigate persistent shoulder pain. The ordering physician’s office submits the claim three days later, expecting standard reimbursement.
Here’s the catch: this particular payer requires prior authorization for all non-emergency MRIs, and nobody on the front-end team checked that requirement before scheduling the scan.
The remittance advice comes back with CO 197 paired with remark code MA120, meaning no authorization exists on file anywhere.
The billing team pulls the patient’s chart, confirms the MRI was medically necessary, and contacts the payer to request retroactive authorization. The payer approves it within five business days.
The claim gets corrected, resubmitted with the new authorization number, and paid in full three weeks later.
This is exactly how most CO 197 denials resolve: not through panic, but through a calm, methodical paper trail.
Who Is Responsible for Paying a CO 197 Denial?
Let’s answer this one directly, because it’s the question that worries people most.
The provider is responsible for a CO 197 denial, not the patient. That’s the entire point of the “CO” prefix.
You cannot send the patient a bill for this amount. Your contract with the insurance company already states that missing authorization is the provider’s responsibility to resolve.
Your only real paths forward are fixing the claim, appealing it, or absorbing the cost as a write-off.
X12, CARC, and RARC: The Standards Behind Denial Codes
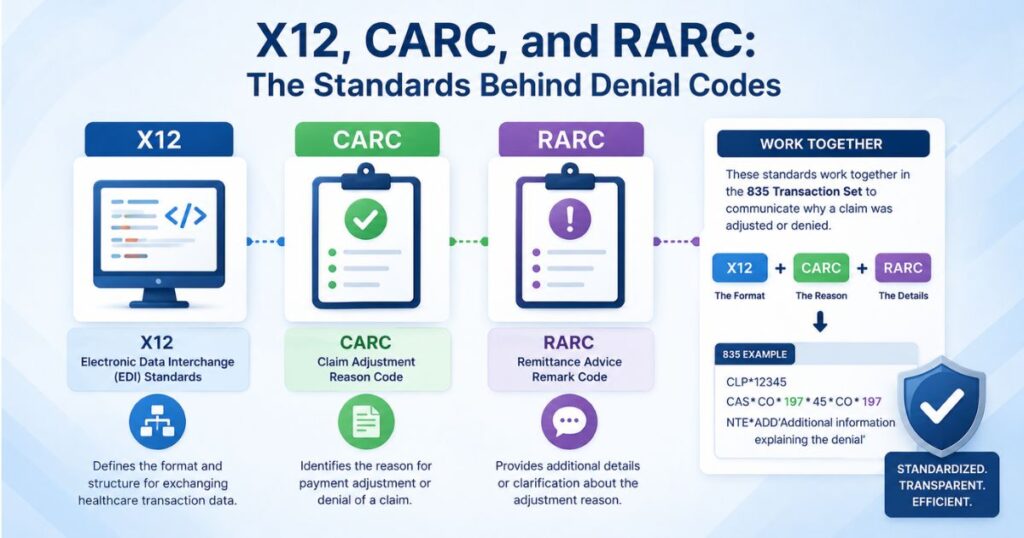
Ever wonder who actually decides what these codes mean? It’s not random, and it’s not made up by each insurance company individually.
X12 is the official organization, chartered by the American National Standards Institute, that creates and maintains these codes for the entire healthcare industry. Every payer in the country uses the same standardized list.
That’s where CARC (Claim Adjustment Reason Code) comes from. It’s the official category that CO 197 belongs to.
RARC (Remittance Advice Remark Code) is the companion system that adds extra detail. Remember N210, MA120, and M62 from earlier? Those are all RARCs, working alongside the CARC to paint the full picture.
Knowing this distinction makes you faster at reading any denial, not just CO 197.
Conclusion
The CO 197 Denial Code typically means that a healthcare service is excluded from coverage or fails to meet the insurer’s medical necessity or policy requirements. To resolve this denial, providers should verify patient benefits, review payer policies, submit supporting documentation if needed, and appeal the decision when appropriate. Proper eligibility checks before treatment can help prevent future CO 197 denials.
FAQs
What does CO 197 mean on my EOB?
It means the insurance company didn’t receive prior authorization or notification before your service was performed. The provider, not the patient, is responsible for resolving it.
Can a patient be billed for a CO 197 denial?
No. Because it’s coded as a Contractual Obligation, the provider must absorb the cost, appeal the decision, or correct the claim. The patient cannot be billed for this amount.
What is the difference between CO 197 and PR 197?
Both mean authorization was missing, but CO 197 makes the provider responsible for payment, while PR 197 shifts that responsibility to the patient under specific plan terms.
How long do I have to appeal a CO 197 denial?
Appeal windows vary by payer, but most range from 30 to 180 days from the denial date. Always check your specific payer’s policy manual to confirm the exact deadline.
What is the remark code N210?
N210 is a code that often accompanies CO 197. It simply tells you that you have the right to appeal the decision, which is good news if you have the documentation to support your case.